In a world where mental health conversations have finally entered the mainstream, the gap between awareness and genuine, clinically rigorous care remains dangerously wide. Services are overwhelmed, diagnostic backlogs stretch for years, and too many adults are still being treated for the surface while the architecture underneath goes unseen. It is within this strained landscape that Dr Sai Achuthan, Consultant Psychiatrist and Founder of Insight Diagnostics, has emerged as a transformative voice. With a career built on an unusual blend of deep clinical expertise, cross-cultural insight, and entrepreneurial vision, he is reshaping how neurodevelopmental conditions like autism, ADHD, and their combined presentation are recognised and understood in adults.
From his consulting rooms to his international supervision work in the West Bank and Gaza, and through his books, including Unmasking Autism, Dr Sai brings a philosophy as precise as it is compassionate: accuracy is kindness, the person is not the diagnosis, and mental health care must be cross-cultural by design.
As Chair of the Royal College of Psychiatrists South West Division and a recognised figure among the UK’s Top 100 Influential People, his credibility is anchored not in titles but in the thousands of quiet moments where a patient finally hears the words that let them set down decades of self-blame. This is the story of a leader who refused to wait for the system to catch up and instead built something faster, kinder, and clinically uncompromising.
From Malaysia to the world, a mental health journey built on deep listening
Dr Sai Achuthan’s path into psychiatry was never a straight line, and that is precisely what made it meaningful. After qualifying in Malaysia and completing his UK training, he layered specialism upon specialism: Addiction Medicine, an MSc in Clinical Psychiatry, an MBA, leadership diplomas, MRCPsych, and a Senior Fellowship in Medical Leadership. He also received an Hon PhD in Advanced Science, is completing his Master’s in Psychology, and in 2026 was awarded the MSc Psychology Honoris Causa, the highest honour the University of Plymouth Marjon can bestow.
Drawn to psychiatry by the conviction that nowhere else in medicine do you truly understand a person, Dr Sai built a career meeting lives rather than treating presentations. This belief carried him to neurodevelopmental psychiatry, where he founded Insight Diagnostics Global after watching adults wait years for assessments while their careers and self-worth unravelled, determined to build something faster, kinder, and clinically uncompromising on a global scale.
The thousand small moments that redefined psychiatry’s purpose
There is a particular silence that fills the room when someone in their late thirties or forties finally hears, “Yes, you are autistic,” or “Yes, this is ADHD,” and then they cry. Dr Sai Achuthan has witnessed this countless times. His defining career moment is not a single turning point but the quiet accumulation of these thousand small ones. What moves him is not the diagnosis itself, but what the tears represent: decades of self-blame finally falling away. This has reframed his understanding of psychiatry. It is not merely symptom management; it is the quiet, profound restoration of a person’s self-understanding.
Alongside these intimate clinical encounters, another defining thread has woven itself through his career: the experience of working internationally. Sitting with families across vastly different cultural contexts, and most recently supervising consultants and trainees in the West Bank and Gaza, has revealed something both simple and urgent. The conditions are the same the world over, but the recognition is not. That gap between the universality of neurodevelopmental struggle and the stark inequality of access to diagnosis is what he has dedicated his career to closing.
The real picture of mental health today
Walk into any psychiatry clinic today, and you will feel a system straining under demand it was never built to handle. Dr Sai sees three crises colliding: adult neurodevelopmental conditions are finally visible, but services have not kept pace; anxiety and burnout are rising sharply among professionals masking neurodivergence, and addiction has evolved beyond substances to include screens, work, and validation, becoming deeply entangled with the other two crises.
Socially, the challenge is equally complex. Mental health has been popularised, which is a genuine step forward, but it has also been flattened and commodified. Self-diagnosis through social media has filled the gap left by under-resourced services, empowering some, yet risky when it entrenches the wrong narrative. For Dr Sai Achuthan, the path forward is clear: keep the bar of clinical rigour high while keeping the door of access wide open. Neither can be sacrificed for the other.
The case that changed everything
Early in his consultant career, Dr Sai Achuthan assessed a woman in her forties who had carried the label of “treatment-resistant depression” for fifteen years without any real improvement. Within twenty minutes of taking a proper developmental history that went beyond sleep and appetite, the picture transformed completely. She was autistic with co-occurring ADHD, and what had been labelled as depression was in fact lifelong autistic burnout and rejection sensitivity dressed up as low mood. Nobody had ever asked about her childhood, her sensory experiences, or how she navigated friendships; they had only ever asked about the surface.
That single case crystallised something Dr Sai Achuthan carries into every consultation since: in adult psychiatry, we are still far too often treating the surface and missing the architecture underneath. It changed how he takes a history, how long he takes, and most importantly, how he now trains others to do the same. The questions nobody thinks to ask are often the ones that unlock everything.
Three principles that guide every consultation
Everything Dr Sai Achuthan does rests on three non-negotiable principles. First, the person is not the diagnosis; the diagnosis is a tool the person uses, not a label they live under. Second, accuracy is kindness. A rushed or imprecise assessment is not faster; it is slower, because the person then spends years on the wrong path, internalising the wrong story about themselves. Third, mental health care must be cross-cultural by design, not by afterthought.
Most diagnostic frameworks were built on a narrow demographic, and the field is still discovering how much that has cost women, people of colour, and anyone who does not present in the textbook way. These three convictions: person over label, precision over speed, and cultural humility over assumption form the foundation of every assessment, every training session, and every piece of advocacy he undertakes.
Why the assessment itself is the intervention?
Conventional psychiatry relies on short medication reviews and checklists; Dr Sai Achuthan works the other way round, treating the assessment itself as the intervention. Before a patient arrives, he has read every referral note, questionnaire, and piece of collateral, then takes a full developmental and cultural history using tools like ADOS-2, ADI-R, and DIVA to inform rather than replace his clinical judgement. The tools are guides, not answers, because masking is too complex to be recognised by forms alone.
When faced with complex or long-term presentations, Dr Sai Achuthan works from a single guiding assumption that there is almost always a neurodevelopmental, trauma, or addiction thread running underneath that nobody has yet pulled on, and finding that thread allows the rest of the picture to reorganise itself. It is not about doing more but about looking deeper and understanding that the surface is rarely the whole story.

Why AuDHD stayed invisible for a generation?
For a generation, AuDHD was missed because the system was built around single diagnoses, sending people down either the ADHD or autism pathway and ignoring what lay behind the other door. The two conditions mask each other cleverly: ADHD’s social impulsivity hides autistic social difficulty, while autistic rule-following dampens visible ADHD impulsivity. The result has been decades of missed diagnoses, particularly among women and those who learned to mask early.
A truly integrated assessment looks completely different. It begins with the assumption that both conditions may be present, takes a unified developmental history, and uses tools from both diagnostic traditions in the same encounter. It examines sensory profile, executive function, social cognition, emotional regulation, and reward sensitivity as one coherent picture, not two questionnaires stapled together. Most importantly, it reports back in a way that helps the person understand how the two interact in their daily life, rather than simply listing which boxes they tick.
When autism and ADHD pull in opposite directions?
Imagine building a careful structure each morning to survive the day, only to watch yourself dismantle it by mid-morning. That is the reality Dr Sai’s patients describe most viscerally. Autism pulls toward routine, predictability, and deep focus; ADHD pulls toward novelty, stimulation, and impulsivity. Inside one nervous system, these opposing forces produce a specific kind of exhaustion, leaving the person blaming themselves for being lazy or scattered when they are actually mediating an internal civil war few can see.
Treatment cannot be generic. Stimulant medication can quiet ADHD but may sharpen rigidity or amplify sensory overload in someone with autistic features. Dr Sai Achuthan titrates slowly, monitoring attention alongside flexibility and sensory tolerance, and combines medication with coaching, environmental design, and therapy that addresses both profiles. The goal is never to flatten either trait but to help the two coexist without burning the person out.
Too sociable, too emotional, too successful
Dr Sai Achuthan co-authored Unmasking Autism: The Cross-Cultural Revolution in Adult Assessment after years of watching the same heartbreaking scene: an intelligent, articulate adult, often a woman from a minority background, told for decades that she could not be autistic because she was too sociable, too emotional, too successful, or simply too female. Every one of those statements, he insists, is wrong, and the diagnostic frameworks that produced them are wrong too.
Most diagnostic tools were normed on white, male, middle-class samples, leaving cultural fingerprints unrecognised. Dr Sai Achuthan believes assessors need cultural humility, longer histories, and the skill to recognise masking as survival, not non-autism. The next generation must hold the diagnostic frame open rather than shutting it when someone smiles or holds down a job, because those are often the very reasons the diagnosis was missed.
Lessons from the West Bank and Gaza
Through the Royal College of Psychiatrists, Dr Sai supervised ADHD and ASD assessment training in the West Bank and Gaza, work he calls among the most significant he has ever done. The conditions are universal, presenting exactly as they do in the UK or Malaysia. The real obstacles are the surrounding system: limited specialists, deep-rooted stigma, war disrupting developmental histories, and a desperate shortage of assessment tools and supervision.
What moved him most was the extraordinary appetite among local clinicians, who sat in supervision sessions under unimaginable conditions, taking notes and asking sophisticated questions with utter determination. It reinforced his core belief that neurodevelopmental care cannot be a luxury reserved for high-income countries, and he intends to keep contributing for as long as he is able.
Busting myths and building trust
The misconceptions Dr Sai Achuthan encounters daily are depressingly basic: that ADHD is a children’s condition, that autism means no eye contact or relationships, that having a job or family rules out either, and that adult diagnosis is too late to matter. He builds trust by reading every note, asking the questions nobody has asked, never rushing, naming masking when he sees it, and writing reports that reflect the person’s actual life rather than a templated document. When patients feel truly seen, they trust the process, whatever the outcome.
Building credibility through work, not titles
Dr Sai Achuthan’s contributions span clinical practice, leadership, academic writing, and public speaking, with recognition following the work rather than driving it.
His key contributions include:
- Authorship: He has written three books in neurodevelopmental psychiatry: The Bridge Builder, Unmasking ASD: Cross-Cultural Differences, and Adult ADHD Guidelines, each designed to translate complex clinical thinking into guidance that both clinicians and patients can genuinely use.
- National Leadership: Chair, Royal College of Psychiatrists South West Division, Chair, Approval Panel, Approved Clinicians, Section 12 doctors, Midlands and East, national training and standards.
- Senior Clinical Leadership: Medical Director, Deputy Regional Medical Director, independent mental health organisations, co-chaired, national education programme, specialty doctors.
- International Education: Journal reviewer, international conference speaker, Global ADHD Conference, educator of consultants and trainees, supervision work, West Bank and Gaza, Royal College of Psychiatrists.
- Awards and Recognition: Consultant of the Year (2023), finalist for Educator of the Year (2023 and 2024), Medical Director of the Year (2024), Top 100 Influential People in the UK (2025), and international Trailblazer Leader to Watch (2025).
The evolution of impact
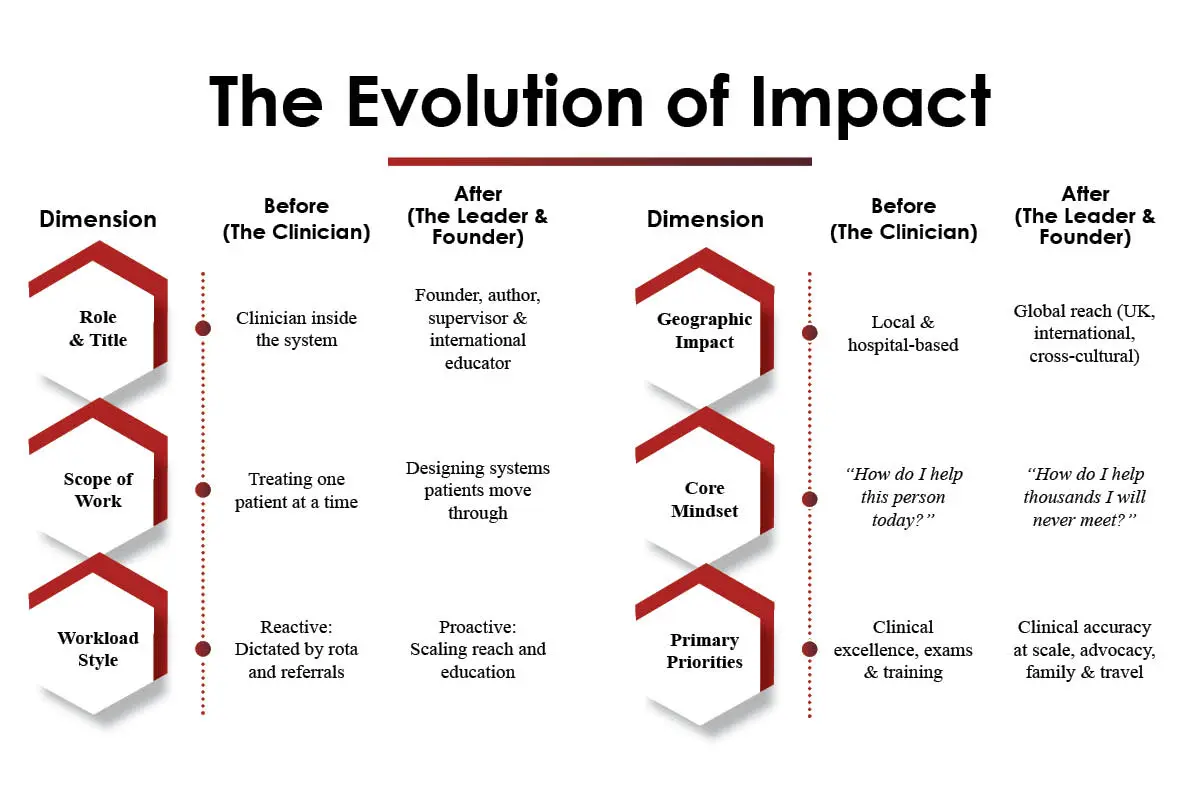
| Dimension | Before (The Clinician) | After (The Leader & Founder) |
| Role & Title | Clinician inside the system | Founder, author, supervisor & international educator |
| Scope of Work | Treating one patient at a time | Designing systems patients move through |
| Workload Style | Reactive: Dictated by rota and referrals | Proactive: Scaling reach and education |
| Geographic Impact | Local & hospital-based | Global reach (UK, international, cross-cultural) |
| Core Mindset | “How do I help this person today?” | “How do I help thousands I will never meet?” |
| Primary Priorities | Clinical excellence, exams & training | Clinical accuracy at scale, advocacy, family & travel |
A day in a leader’s life: the rhythm behind the work
Dr Sai’s routine mirrors what he advises AuDHD patients, building routine and predictability to anchor the mind with novelty built in to stay engaged, because without that scaffold, the day collapses and with it he does his best work.
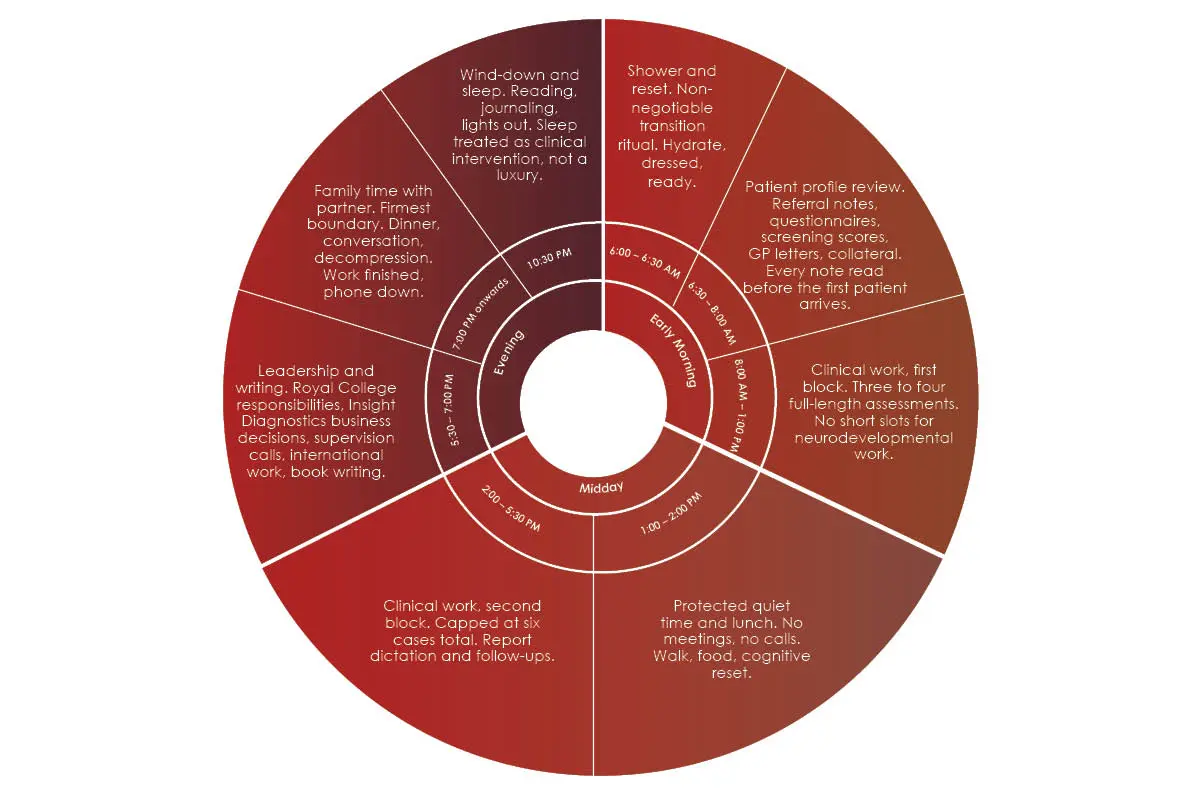
- 6:00 AM — Wake up. Same time every day, weekdays and weekends. No snooze, no negotiation.
- 6:00 – 6:30 AM — Shower and reset. Non-negotiable transition ritual. Hydrate, dress, ready.
- 6:30 – 8:00 AM — Patient profile review. Referral notes, questionnaires, screening scores, GP letters, collateral. Every note is read before the first patient arrives.
- 8:00 AM – 1:00 PM — Clinical work, first block. Three to four full-length assessments. No short slots for neurodevelopmental work.
- 1:00 – 2:00 PM — Protected quiet time and lunch. No meetings, no calls. Walk, food, cognitive reset.
- 2:00 – 5:30 PM — Clinical work, second block. Capped at six cases total. Report dictation and follow-ups.
- 5:30 – 7:00 PM — Leadership and writing. Royal College responsibilities, Insight Diagnostics business decisions, supervision calls, international work, book writing.
- 7:00 PM onwards — Family time with partner. Firmest boundary. Dinner, conversation, decompression. Work finished, phone down.
- 10:30 PM — Wind down and sleep. Reading, journaling, lights out. Sleep is treated as a clinical intervention, not a luxury.
- Weekends — Occasional work, mostly travel. 44 international trips. Cross-cultural perspective and antidote to clinical intensity.
Featured recognition and a message for those still suffering in silence
Dr Achuthan Sai’s work has been featured across several prominent platforms, and his message to those still struggling is one he delivers with the same care he brings to every consultation.
1. Features and recognition:
- Professional pages: Insight Diagnostics Global Top Doctors, Harley Mind Care, ADHD Health Clinic, Psych-UK, ADHD Clinics
- Insight Success: “Trailblazer Leader to Watch, 2025”
- CXO Time: “Iconic Leader to Watch, 2025”
- Top 100 Influential People in the UK listing for 2025 and 2026
2. A message to those silently struggling:
To anyone who has not yet asked for help, Dr Sai’s message is simple: you are not alone, and you are not as broken as you fear. The hardest step is speaking up, but that single act changes everything. You do not need the perfect words, just the willingness to be heard. Find one trusted person and begin there. The rest is the clinician’s job.

Advice for the next generation of mental health professionals
The field of psychiatry does not change because institutions decide it should but because individuals refuse to wait for permission, and that is the conviction Dr Sai Achuthan offers young psychiatrists and aspiring advocates.
His guidance rests on three pillars drawn directly from his own journey:
- Be a clinician before you are anything else. Leadership, writing, and advocacy all rest on the credibility of being genuinely good at the consultation. Master the assessment, and everything else follows.
- Take cultural humility seriously. The diagnostic frameworks you were trained on were built by a narrow group of people; the patients you will serve are not. Read widely, travel if you can, and be willing to be wrong about what “typical” looks like.
- Build the system rather than simply surviving it. If you see a gap, start something and do not wait for permission, because the field changes when individuals decide it should, and the next generation must be those individuals.
Key takeaways:
- The assessment itself is the intervention; rush it, and the person spends years on the wrong path.
- The person is not the diagnosis; a label is a tool to be used, not an identity to live under.
- Accuracy is kindness; precision in diagnosis is not pedantry; it is the deepest form of respect.
- Beneath every complex presentation lies a neurodevelopmental, trauma, or addiction thread that nobody has yet pulled on.
- Cultural humility is non-negotiable; diagnostic tools built on narrow demographics will keep missing those who don’t present in the textbook way.
- Build the system, don’t just survive it; if you see a gap, start something, and don’t wait for permission.